Herniated Disc vs. Bulging Disc: What's the Difference, and Do You Actually Need Surgery?
If you've been told you have a "disc problem" in your back, you probably left the appointment with more questions than answers. Maybe your doctor said "bulging disc." Maybe they said "herniated." Maybe they used the words interchangeably — which happens more often than it should — and you walked out unsure whether you're dealing with something that will resolve on its own or something that requires surgery.
You're not alone in that confusion. Disc-related diagnoses are among the most common reasons people seek treatment for back pain, and the terminology can feel overwhelming. But understanding the actual difference between a herniated disc and a bulging disc matters — because it affects what treatment you need, how urgently you need it, and whether surgery should even be part of the conversation.
At Platinum Healthcare Physical Medicine in Sarasota, we've treated hundreds of patients with disc injuries over nearly two decades. The vast majority of them did not need surgery. Here's what you need to know.
The Anatomy of a Spinal Disc: A Quick Foundation
Before comparing the two conditions, it helps to understand what a spinal disc actually is and what it does.
Your spine is made up of 33 vertebrae — the bony segments stacked on top of each other from your skull to your tailbone. Between most of those vertebrae sits an intervertebral disc, a round, flat structure that serves as a shock absorber. Each disc has two parts.
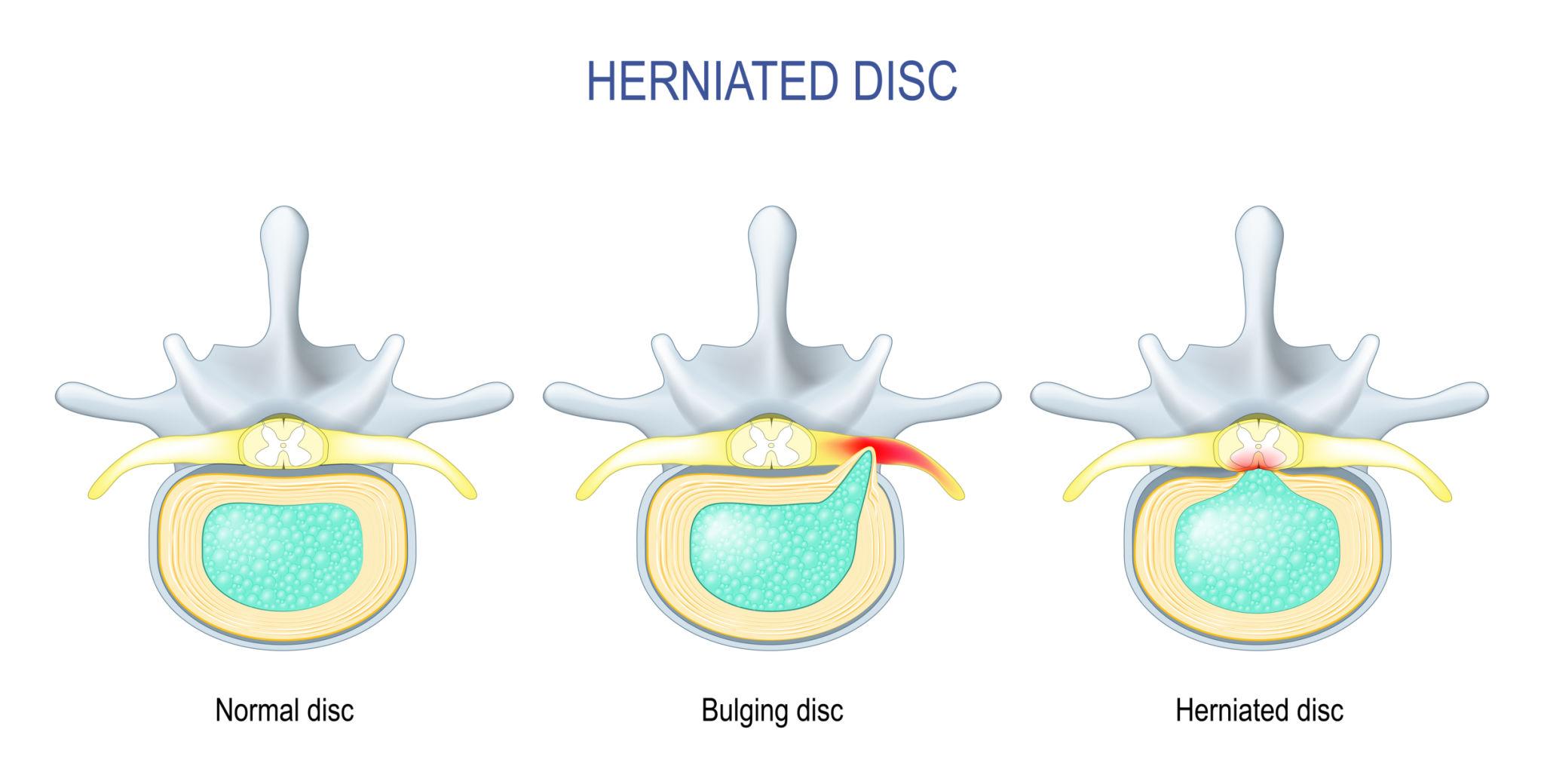
The annulus fibrosus is the tough outer layer. It's made up of multiple rings of strong cartilage fibers arranged in overlapping layers, almost like the plies of a radial tire. This outer wall gives the disc its shape, holds it in place between the vertebrae, and protects what's inside.
The nucleus pulposus is the soft, gel-like center. It's composed mostly of water and collagen and has a consistency similar to thick jelly. This inner core is what gives each disc its ability to compress and rebound — absorbing the forces of walking, bending, twisting, and even just sitting upright.
When both components are healthy and intact, the disc functions like a perfectly sealed hydraulic cushion. Problems start when the structure begins to break down — and how it breaks down determines whether you have a bulging disc or a herniated disc.
What Is a Bulging Disc?
A bulging disc occurs when the disc loses some of its normal height and shape — usually due to age-related dehydration and wear — and the outer wall extends outward beyond its normal boundary. The key distinction is that the annulus fibrosus is still intact. Nothing has torn. Nothing has leaked. The disc has simply flattened and spread, the way a hamburger patty that's slightly too wide hangs over the edge of the bun.
Bulging discs are extremely common. Studies using MRI imaging on people with no back pain have found that a significant percentage of adults over 40 have at least one bulging disc and don't even know it. In many cases, a bulging disc produces no symptoms at all.
When a bulging disc does cause problems, it's typically because the outward protrusion is pressing on a nearby nerve root or narrowing the spinal canal. Symptoms tend to develop gradually and may include dull, aching pain in the lower back or neck, stiffness and reduced range of motion, and mild numbness or tingling in the arms or legs depending on the location of the affected disc.
Bulging discs are usually considered a normal part of spinal aging. They deserve attention, but they rarely require urgent intervention — and they almost never require surgery.
What Is a Herniated Disc?
A herniated disc is a more significant structural failure. In this case, the outer wall of the disc — the annulus fibrosus — has developed a crack or tear, and the soft inner material (the nucleus pulposus) has pushed through that opening and into the spinal canal.
The analogy here is a jelly doughnut being squeezed until the filling leaks out. Once that gel-like material escapes the disc, it can directly compress a spinal nerve root or even the spinal cord itself. On top of the mechanical pressure, the nucleus pulposus is chemically irritating to nerve tissue — meaning the leaked material can trigger inflammation and pain even without significant compression.
This is why herniated discs tend to produce more intense and immediate symptoms than bulging discs. Depending on the location of the herniation, you might experience sharp, shooting pain down one leg (sciatica) if the herniation is in the lumbar spine, radiating pain into the shoulder, arm, or hand if it's in the cervical spine, localized burning or electric-shock sensations, noticeable muscle weakness in the affected limb, or numbness and tingling that follows a specific nerve pathway.
Herniated discs are one of the most common causes of sciatica in adults between 30 and 50. They can result from a single event — a lifting injury, a car accident, a sudden twist — or from the gradual progression of a disc that was already weakened by degeneration.
In rare but serious cases, a large herniation can compress the bundle of nerves at the base of the spinal cord (the cauda equina), causing symptoms like sudden loss of bladder or bowel control, numbness in the groin area, or progressive weakness in both legs. This is a medical emergency that does require surgical intervention. But it accounts for a tiny fraction of herniated disc cases.
The Most Important Takeaway: Neither Diagnosis Automatically Means Surgery
This is the message we want every patient to leave with. A bulging disc or a herniated disc on your MRI does not mean you need an operation.
The majority of disc injuries — both bulging and herniated — improve with conservative, non-surgical treatment. Research consistently shows that most patients with disc herniations experience significant improvement within six to twelve weeks of appropriate non-surgical care. For bulging discs, the timeline is often even shorter.
The problem is that when you're in pain — especially the kind of radiating, nerve-compressing pain that a herniated disc can produce — it feels urgent. And when a surgeon shows you an MRI image and points to the disc material pressing on your nerve, surgery can seem like the obvious answer. But surgery carries its own risks, and the outcomes aren't guaranteed. Failed back surgery syndrome affects an estimated 20% to 40% of spinal surgery patients, and success rates decline significantly with each subsequent procedure.
That's why exploring conservative treatment first isn't just a reasonable option — it's what most clinical guidelines actually recommend.
Just got a disc diagnosis and not sure what to do next? Call Platinum Healthcare at 941-927-1123 for a free screening. We'll review your imaging and explain your non-surgical options.
How Platinum Healthcare Treats Disc Injuries Without Surgery
At Platinum Healthcare, herniated disc treatment in Sarasota starts with understanding exactly what's going on. Not every disc injury is the same, and a one-size-fits-all approach doesn't work. Our team evaluates the type of disc involvement (bulging vs. herniated vs. sequestered fragment), the location (cervical, thoracic, or lumbar), and the degree of nerve involvement before building a treatment plan. Here's what that plan typically includes.
Spinal Decompression Therapy
This is often the centerpiece of our disc treatment protocol. Spinal decompression uses a specialized motorized table to gently stretch the spine, creating negative intradiscal pressure — a controlled vacuum effect within the affected disc. This negative pressure serves two purposes: it encourages bulging or herniated disc material to retract back toward the center of the disc, and it promotes the flow of oxygen, water, and nutrients into the disc to support healing.
Unlike surgical decompression (which involves removing bone or disc tissue), this is entirely non-invasive. There's no anesthesia, no incision, and no recovery period. Patients typically lie comfortably on the table for 20 to 30 minutes per session, and many report relief within the first several treatments.
Spinal decompression for herniated disc injuries in Sarasota is one of the most requested services at our clinic — and for good reason. It directly addresses the mechanical problem without any of the risks associated with surgery.
Learn more about Spinal decompression.
Chiropractic Adjustments
Disc problems rarely exist in isolation. A herniated disc in the lumbar spine is often accompanied by — and sometimes caused by — misalignment in the surrounding vertebral segments. When the spine is out of proper alignment, it places uneven mechanical load on the discs, accelerating wear on one side and increasing the likelihood of a bulge or herniation.
Our chiropractors use targeted, precise adjustments to restore proper alignment and take abnormal pressure off the affected disc. This doesn't just address the symptom — it addresses one of the structural factors that caused the disc to fail in the first place.
Learn more about chiropractic adjustments.
Physical Rehabilitation
A disc that's been decompressed and realigned still needs a stable foundation to stay healthy long-term. That foundation is the muscular system surrounding the spine — the deep core stabilizers, the paraspinal muscles, the hip and pelvic floor musculature that collectively hold the spine in its proper position under load.
Our physical rehabilitation program is designed to strengthen these supporting structures, improve flexibility, and retrain movement patterns that may have been contributing to disc stress. This is the phase of treatment that prevents recurrence — and it's the step that many patients skip when they rely on surgery or medication alone, which is one of the reasons disc problems so often come back.
Learn more about physical rehabilitation.
When Patients Come to Us After Surgery Has Already Failed
Not every patient walks through our door with a fresh diagnosis. Some come to us after already having disc surgery — a discectomy, a laminectomy, even a spinal fusion — and they're still in pain. This is more common than most people realize. Failed back surgery syndrome is a recognized medical condition, and the patients living with it often feel like they've run out of options.
They haven't. Our team has significant experience working with post-surgical patients whose disc-related pain persisted or returned after an operation. The approach is the same — identify the current source of pain, determine whether residual disc involvement, scar tissue, or adjacent-segment degeneration is driving the symptoms, and build a non-surgical treatment plan to address it.
If you had back surgery and you're still hurting, that doesn't mean the only answer is more surgery. In many cases, it means the root cause wasn't fully addressed the first time — and conservative treatment may be able to reach what the scalpel couldn't.
Learn more about Failed back surgery syndrome.
Get Answers About Your Disc Diagnosis in Sarasota
Whether you've just been told you have a bulging disc, you're dealing with the sharp nerve pain of a herniation, or you're living with pain after a disc surgery that didn't deliver the results you were promised — we want to help you understand your options.
Platinum Healthcare Physical Medicine offers free screenings for patients with disc-related pain at our office on Bee Ridge Road in Sarasota. We serve patients throughout Sarasota, Bradenton, Lakewood Ranch, Venice, Osprey, and the surrounding communities.
Bring your MRI. Bring your questions. We'll give you honest answers about what we see, what we think is causing your pain, and whether non-surgical disc treatment can work for you.
Call us today at 941-927-1123 to schedule your free screening. A disc diagnosis doesn't have to end with surgery.